
Prevent CKD progression
- use claims data to track behavior change and quantify the effectiveness of the awareness letter
In part 2, we share the evaluation methods and results of this project, future developments, and thoughts on collaboration.
(You can read Part 1 from here)
How is a "doctor visit" defined? Data is used to establish outcomes and the control group
―― Could you tell us how you evaluate behavior change?
Kento Takeyama:We use the health insurance claims data for the three months after the letter is sent to evaluate whether or not the patient has visited a doctor. However, it was very difficult to determine what constitutes a "doctor visit," since CKD is rarely diagnosed at the first visit.
Therefore, we extracted data on those with a confirmed diagnosis of CKD from our anonymous claims database of approximately 1.2 million patients, analyzed the patient journey until the diagnosis was made, and after discussions with specialists and AstraZeneca colleagues, defined outcomes as "biochemical test performed," "lifestyle disease-related diagnosis" and "kidney disease-related diagnosis."
Another important point is that we found people who were close to the target population from the data and created a control group.
Lei Liu:For example, even if we find out that "30% of the people who received the disease awareness letter visited a doctor," we don't know how we should evaluate that, do we? Because some people will see a doctor for some reason without any kind of campaign. We can only clarify the impact by comparing the results with those of the control group.
Takeyama :Use data to define outcomes. Evaluate the impact in the control and intervention groups. I believe that these are all unique points that PREVENT has been able to achieve through our accumulated expertise.

―― Could you share the main results?
Takeyama :In the control group (n=6660), 26.0% (n=1731) had biochemical tests performed, 32.9% (n=2191) had lifestyle diseases diagnosed, and 3.6% (n=239) had kidney disease-related diagnoses. The disease awareness group (n=740) had a 39.7% (n=293) rate of biochemical testing, a 43.0% (n=318) rate of diagnosis of lifestyle diseases, and a 9.2% (n=68) rate of diagnosis related to kidney disease. All outcomes were higher in the disease awareness group.
Liu:Of the 740 subjects, 312 (42%) showed behavior change ,which was more than we had expected. This was one of the results that validated the hypothesis that "patients become aware of the risk, bring the awareness letter to the doctor, the doctor becomes aware of the kidney risk and performs tests, and the test results lead to a kidney disease-related diagnosis," and it also suggested a behavioral change in which doctors perform tests based on the letter brought by the patients. Since the difference between the two groups started to appear from the 0th month after the letter was sent, and the difference gradually increased, it would be very interesting to see what the results would have been if we had followed up longer.
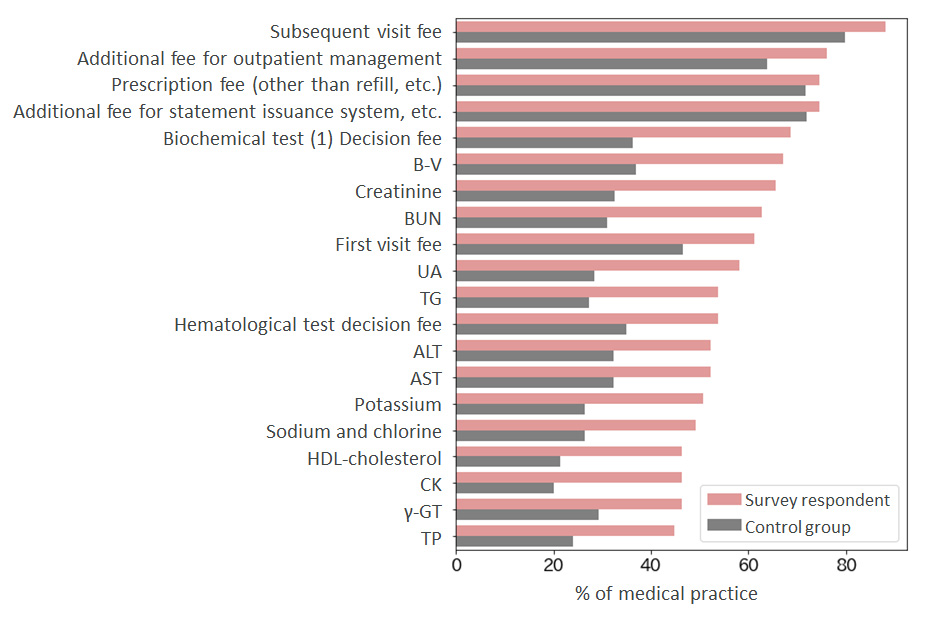
●Outcome assessment
Medical practice among survey respondents who have seen a doctor or plan to see a doctor vs. control group
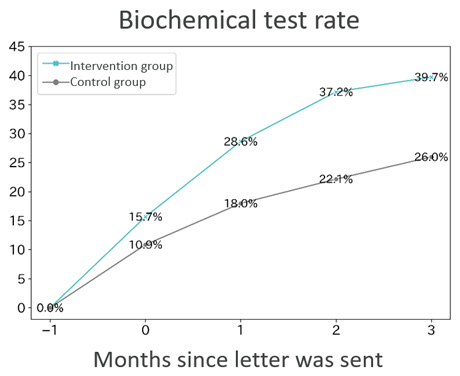
●Outcome results (Testing rate)
Comparative analysis of biochemical testing rates (urine, feces, and blood) based on claims data in the intervention and control groups
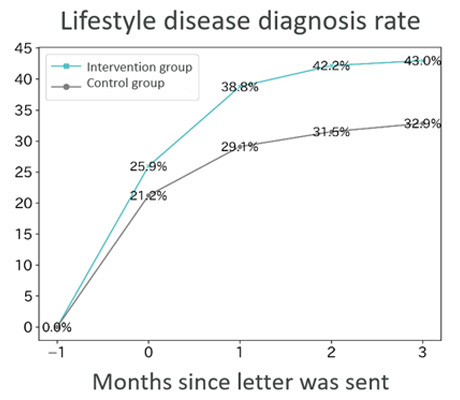
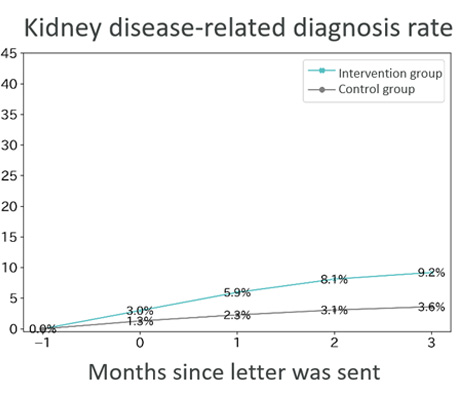
●Outcome results (name of lifestyle disease and kidney disease-related diagnoses)
Comparative analysis of rates of lifestyle disease-related diagnoses1 and kidney disease-related diagnoses based on claims data in the intervention and control groups
―― Are there any challenges that you see in the process or results?
Takeyama :Behavioral change varied by group. For example, we were not able to encourage those who "have not been to a hospital in the past year" to see a doctor. Additional measures for this segment of the population need to be further explored.
Liu:In the so-called "bedrock segment," who are at high-risk and need early behavioral change, we did not see behavioral change in this project either. We recognize that this is another issue that we need to continue to consider. In the meantime, it is difficult to clearly track the results of conventional disease awareness activities such as TV commercials and public lectures. For the first time, this project allowed us to quantify the results of our efforts. We can discuss ROI (Return on Investment) and say that we now have a KPI (Key Performance Indicator) for continued investment in disease awareness activities.
“Win x 4” model for both scale-up and rollout to other diseases

―― What are your future plans?
Liu:For example, we are considering scaling up the project to see if behavior change can occur in a larger group. Also, CKD has a long course and it is difficult to continue to follow patients for a long time, so we are considering building a model that can predict medium- to long-term risk using historical data.
Takeyama :For this project, we selected the target population based on the definition, but for the future, we have several hypotheses and are discussing with AstraZeneca colleagues how to work on them.
Liu:If we can achieve this, we expect that the scheme will be used more widely by health insurance association and national health insurance.
What is important is to contribute to the early detection of CKD. We want to create a sustainable model.
―― Is it possible to apply it to diseases other than CKD?
Takeyama :If the disease is such that the right patients can be found from the health checkup or claims data, it is possible to roll out to other diseases.
Liu:Of the diseases my team is working on, it can be rolled out to respiratory and liver diseases. There are a number of diseases that have a long course, with low risk awareness in mild cases, and can be diagnosed early through disease awareness.
Takeyama :The fact that we were able to raise awareness of diseases other than lifestyle diseases gave us confidence and reaffirmed the significance of disease awareness. In order to optimize medical costs and improve the quality of life of the insured, we would like to target a wider range of insurers and promote disease awareness for diseases other than lifestyle diseases.
―― What do you think is the motivation and significance of this project?
Takeyama :PREVENT is a startup that implements a system to support "ichi-byo sokusai," which means people can live a healthier life while coping with a disease. This disease awareness campaign is the embodiment of that vision, and we are very proud of the results we have achieved!
Liu:I think we have created a prototype for AstraZeneca's "patient-centered business model.” By providing accurate information to patients, we can make them aware of their own risks and encourage them to take action. It is very significant that we were able to present this model with evidence.
Takeyama : It has become a “win x 4” business, which makes patients, insurers, AstraZeneca and PREVENT happy.
Liu:For i2.JP, we want to introduce this as the first model that we can scale up.
―― What do you think are the advantages of your partner and the attractiveness of i2.JP that you have found through the collaboration?
Takeyama :Bigger companies often perceive startups as vendors. That is not wrong, but Liu-san saw the same issues from the same perspective as a partner, and he was actively involved in the project. We felt very comfortable working together, happy and grateful.
Liu: Partners are partners, not vendors, aren’t they? I believe that only when we work on an equal footing can we reap the benefits of collaboration, and create synergies that take advantage of each other's strengths.
Takeyama-san and everyone at PREVENT are truly outstanding in terms of the quality of their proposals and the depth and breadth of their insights. They are all professionals, and I could tell that they are all sincerely committed to their mission of “making society healthier.”
Takeyama :I think it is rare and fantastic that a pharmaceutical company is leading such a broad open innovation project as i2.JP. Two months after we joined i2.JP, it was decided to launch this project. We want to continue to propose new ideas.
Liu:What started out as a small group of seven companies and organizations has grown to include the public, private, and academic sectors, and is still growing. From now on, we want to collaborate with multiple stakeholders.
If we are to roll out this project in society and turn it into a sustainable model, two companies alone will not be enough. We want to involve more stakeholders to make it sustainable, and we want to grow i2.JP to do that.
※The information in this article was current at the time of the interview. Please note that affiliations, etc. may differ from today.
For inquiries
Interested in joining us?
Thank you for your interest. We will get in touch soon.